Authored by Charlie Lonardo VP, Digital Client Engagement
When Medicare capped annual drug spending at $2,000, the promise sounded simple: affordability, predictability, and relief. But the early data from two very different therapy areas—cardio-metabolic care and immunology—suggest the MPPP is less a fix and more a fault line, exposing where the system bends… and where it breaks.
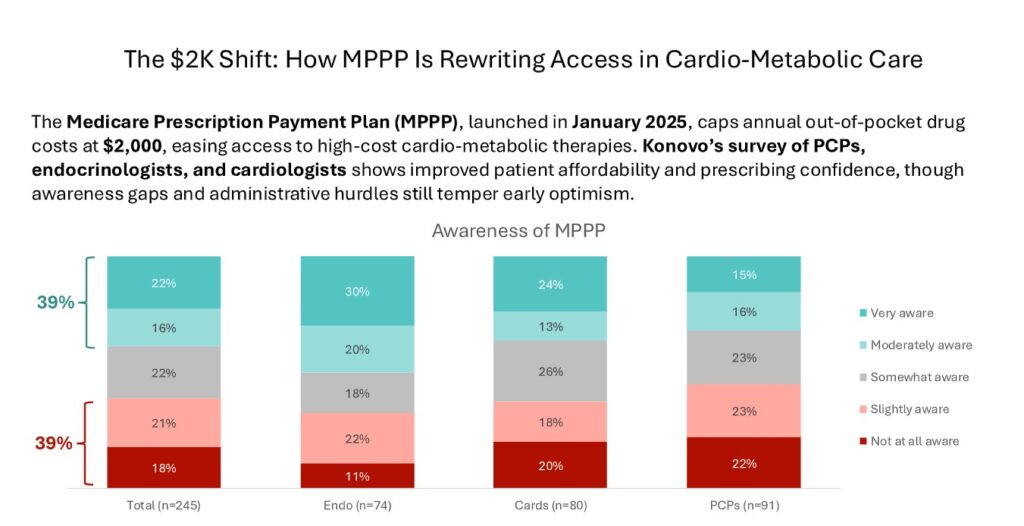
In cardio-metabolic care, enthusiasm is visible but uneven. Cardiologists and endocrinologists report a notable boost in confidence prescribing branded therapies—GLP-1s, SGLT2s, PCSK9s, even siRNAs—now that patients face a clearer ceiling on cost. Some physicians say it’s finally “easier to prescribe medications that cost more,” and early indicators show patient interest rising, even shifting some away from compounded GLP-1s.
And yet 40% of PCPs say patients are not reporting better access or satisfaction. Many still can’t afford the high upfront monthly costs before they reach the $2,000 threshold. Further, some PCPs find themselves in the position of coaching patients on how the system works and there is a general sense of confusion from patients. The MPPP is helping—but only in spurts, and only for some.
Immunology tells the opposite story. Here, the cap appears to be a genuine unlock. Nearly two-thirds of rheumatologists say affordability discussions have improved, and about 40% report they’re now more willing to prescribe higher-cost biologics—a major shift for a specialty where adherence often collapses under cost pressure. Patients seem to feel it too: 58% report perceived improvements in access or satisfaction, far higher than in cardio-metabolic care.
And yet in both fields, the data points to the same stubborn obstacle: bureaucracy. Prior authorizations, formulary exclusions, inconsistent payer rules, and administrative burden—these remain the true gatekeepers. Perhaps the anticipated trends in direct-to-cash in 2026 will impact this?
The early takeaway? The MPPP isn’t transforming care — it’s revealing how the system actually works.
For immunology, financial relief lifts clinical potential. For cardio-metabolic care, affordability shines a light on workflow friction and payer inconsistency. And for healthcare overall, it’s a reminder that reforms don’t change behavior on their own—the system around them must evolve too.
The $2,000 cap is only the beginning. The real test is whether the rest of the system can keep up.